

The Taskforce was founded in 2005 on behalf of AGLA, since then directed by Michel Romanens, MD, and issued scientific statements on coronary risk prediction. The aim of the taskforce is to review current knowledge about this topic and to transfer this knowledge to Swiss Atherosclerosis.
Scientific Statements
Risk and Statistics (Romanens, Ackermann, Spence, Darioli, Rodondi, Corti, Noll, Schwenkglenks, Pencina, 2010)
Risk and Ultrasound (Depairon, Romanens, Darioli, 2010)
Risk and MSCT (Romanens, Corti, Depairon, Darioli, Kaufmann, Rodondi, Roffi, Noll, 2013)
Risk and Stress Imaging (Romanens, Corti, Noll, Zellweger, 2009)
Book Chapter / more papers
Kardiovaskuläre Risikovorhersage mit Bildgebung (Romanens, Darioli, 2007, Hans Huber Verlag)
Agenda 2023
Background: atherosclerosis – a disease of arteries – is a leading cause of mortality, morbidity, disability and societal direct and indirect costs in Switzerland.
Detection of patients at risk: currently, SCORE2 and SCORE2-OP should be used as the basic test (providing a prior probability of ASCVD in 10 years). Because of problems both with sensitivity and specificity of SCORE2, additional information from atherosclerosis imaging is required in order to further stratifiy and personalise ASCVD risk. Technically, results from carotid plaque imaging (total plaque area) and coronary calcifications (Agatston score) are used to calculate posttest risk using the Bayes theorem.
Mathematic section: the Bayes theorem calculates the posttest risk using pretest probability = SCORE2 (equal to prevalence) in case the imaging test is positive (PTP pos: e.g. Agatston Score >0, carotid Total Plaque Area > 21 mm2), otherwise PTP neg formula is used.
PTP pos: (PV x SE)/[PV x SE + (1 – PV) x (1 – SP)]
PTP neg: [PV x (1 – SE)]/[PV x (1 – SE) + SP x (1 – PV)]
From the four field table, sensitivity and specificity of a test can be derived: https://www.kardiolab.ch/BayesCalcTab.html
SE= sensitivity, SP = specificity. The following numbers are used:
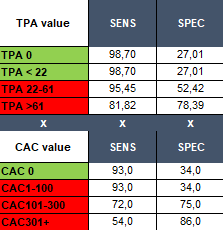
SCORE2/SCORE2-OP with Bayes Theorem Results for TPA and CAC is available as Excel calculator.
Absolute Risk and the Problem of risk categories
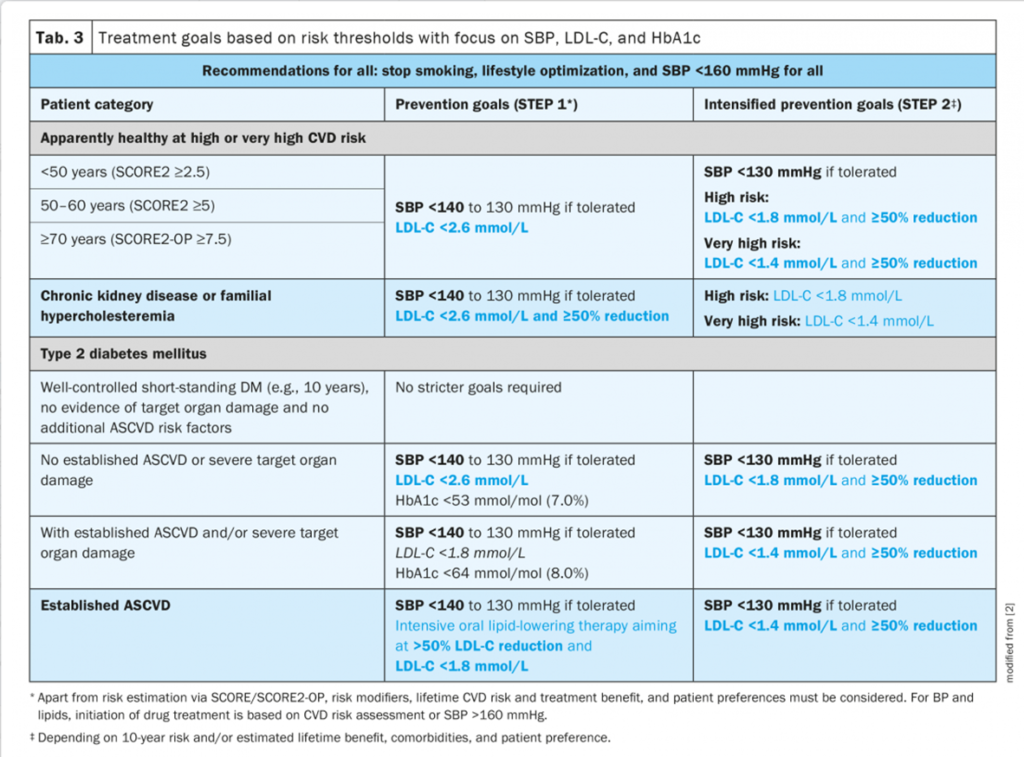
Traditionally, patients are categorised into low, intermediate, high or very high risk of a certain disease, e.g. myocardial infarction or stroke or a combination of both (ASCVD). With SCORE2, risk categories are low-to intermediate, high, very high, and patients are categorized using age and absolute risk (e.g. high risk is present in a person aged < 50 years, if absolute risk is equal or larger than 2.5%):

According to the ESC treatment recommendations 2021, lipid interventions are indicated as presented in the following chart:
Proposition for sequential testing with atherosclerosis imaging of carotid arteries
Since most ASCVD events occur in healthy persons labeled as low to intermediate risk, additional information may be required in order to detect persons with higher risk than expected. As a solution, atherosclerosis imaging using first carotid total plaque are (cTPA) and second coronary calcium scoring as sequential tests on top of SCORE2 results is proposed (literature).
Atherosclerosis Imaging and Women
There is increasing evidence that carotid plaque in women may have two advantages: 1) better risk prediction in women than coronary calcium scores; 2) better risk prediction for incident myocardial infarction in the Tromso Study in women than in man when compared to traditional risk charts. As an example: in the Nixdorf Recall Study with follow-up up to 20 years, in women with ASCVD 10 year risk < 7.5% and CAC <100, 28% of the events occured, while in men, only 9% of the events occurred in this risk category. In the Gudmundsson Study 2022, carotid plaque was directly compared to coronary artery calcificationsin man and women separately (table 2). In women without CAC, 41% had minimal or significant carotid atherosclerosis in the carotid arteries (in men: 21%). In women with CAC, only 5.6% had no carotid plaque (in men: 4.6%). CAC>300 without carotid plaque was found in 0.6% women (in 1.1% men). Therefore carotid plaque is able to detect coronary calcium with a high reliability, findings that have been similar for our Swiss population comparing men and women with CAC and TPA, as seen in our submitted abstracts: TPA is highly prevalent (67%) in female (men: 73%) cardiological patients and of these, 36% had significantly more frequently no CAC than men (22%). More literature.
Atherosclerosis Imaging and cost-effectiveness
Our study showed that carotid ultrasound significantly improved cardiovascular risk stratification and is cost effective. The Swiss Medical Board QALY model presents several drawbacks, which are shown in our sensitivity analysis, where results vary considerably and are not useful for clinical decision making. A “treat them all” strategy with statins in the Swiss population aged 30–65 years may be cost effective, when indirect costs of avoidable cardiovascular events are included, even at an unacceptably low value of a statistical life year.
Atherosclerosis Imaging and credibility of pharmacologic interventions
The concept of treating arteries instead of risk factors has been proposed by David Spence in 2010. In fact, adherence to preventive measures is superior and more credible in patients affected by diseased, atherosclerotic arteries.
Atherosclerosis Imaging and atherosclerosis management
In contrast to coronary calcifications, TPA is reproducible and reliable and should therefore be used to track atherosclerosis over time, e.g. after a year. Since with appropriate and intense prevention, e.g. LDL < 1.8 mmol/l, we observe plaque halting or regression, a process in line with rejuvenation in people aging over the years, that can only be observed reliably with TPA, especially with Statin interventions, as exemplified in a study with patients having carotid stenosis. Spence published a paper in 2003, where patients with plaque stabilisation or regression measured by TPA have an about 50% lower ASCVD risk than patients with plaque progression.
Conclusion
Carotid TPA is a reliable and reproducible tool for the detection and management of atherosclerosis in men and probably even more in women. It is a cost-effective, low-cost, no-radiation, no-software, rapid-training and bedside imaging method that is widely available using linear ultrasound probes. The test is validated and should be incorporated into ASCVD risk detection and management in Switzerland. In contrast to coronary calcification (CAC) measurements with unknown cost-effectiveness, present-radiation and software-dependency and non-bedside testing, cTPA presents undoubtely significant advantages over CAC especially in women.
Papers by Romanens regarding atherosclerosis imaging
Romanens, Michel; Ackermann, Franz; Spence, John David; Darioli, Roger; Rodondi, Nicolas; Corti, Roberto; Noll, Georg; Schwenkglenks, Matthias; Pencina, Michael; ,“Improvement of cardiovascular risk prediction: time to review current knowledge, debates, and fundamentals on how to assess test characteristics“,European Journal of Preventive Cardiology,17,1,18-23,2010,Oxford University Press
Romanens, Michel; Miserez, André R; Ackermann, Franz; Riesen, Walter; Spence, J David; Darioli, Roger; ,Imaging as a cardiovascular risk modifier in primary care patients using predictor models of the European and international atherosclerosis societies,Kardiovaskuläre Medizin,10,4,139-150,2007,
Romanens, Michel; Ackermann, Franz; Abay, Michael; Szucs, Thomas; Schwenkglenks, Matthias; ,Agreement of Swiss-adapted international and European guidelines for the assessment of global vascular risk and for lipid lowering interventions,Cardiovascular drugs and therapy,23,,249-254,2009,Springer US
Romanens, MJ; Berger, DC; Battegay, EJ; ,Predictive value of clinical risk assessment tools and guidelines for 10-year coronary heart disease risk in practice-based primary care,Kardiovaskuläre Medizin,8,5,180-186,2005,
Romanens, M; Ackermann, F; Rothen, J-P; Schwenkglenks, M; Szucs, T; Sudano, I; Corti, R; Noll, G; ,High sensitivity CRP is not a useful tool to further stratify subjects in primary care for their risk of myocardial infarction,EUROPEAN HEART JOURNAL,30,,773-773,2009,“OXFORD UNIV PRESS GREAT CLARENDON ST, OXFORD OX2 6DP, ENGLAND“
Sudano, I; Flammer, AJ; Roas, S; Hirt, A; Kaiser, P; Cantatore, S; Enseleit, F; Romanens, M; Luescher, TF; Ruschitzka, F; ,STRESS-INDUCED VASCULAR DYSFUNTION: EVALUATION OF SYMPATHETIC ACTIVITY AND ENDOTHELIAL FUNCTION IN PATIENTS WITH TAKOTSUBO SYNDROME,JOURNAL OF VASCULAR RESEARCH,50,,22-22,2013,“KARGER ALLSCHWILERSTRASSE 10, CH-4009 BASEL, SWITZERLAND“
Romanens, Michel; Ackermann, Franz; Sudano, Isabella; Szucs, Thomas; Spence, J David; ,Arterial age as a substitute for chronological age in the AGLA risk function could improve coronary risk prediction,Swiss medical weekly,144,2728,w13967-w13967,2014,
Romanens, M; Ackermann, F; Schwenkglenks, M; Szucs, T; Spence, JD; ,Posterior probabilities in sequential testing improve cardiovascular risk prediction using carotid total plaque area,Kardiovaskuläre Medizin,14,,53-7,2011,
Romanens, Michel; Ackermann, Franz; Sudano, Isabella; Szucs, Thomas; Riesen, WF; Darioli, Roger; Schwenkglenks, Mathias; Romanensa, M; Ackermannb, F; Sudanoc, I; ,LDL-cholesterol and the potential for coronary risk improvement,Kardiovaskuläre Medizin,14,,345-50,2011,
Romanens, Michel; Corti, Roberto; Depairon, Michèle; Darioli, Roger; Kaufmann, Beat; Rodondi, Nicolas; Roffi, Marco; Noll, Georg; ,Coronary risk assessment with computed tomography in asymptomatic individuals,Cardiovascular Medicine,16,5,144-52,2013, Depairon, M; Darioli, R;
Romanens, M; ,Cardiovascular risk prediction with ultrasound,Cardiovasc Med,13,09,255-264,2010,
Romanens, Michel; Mortensen, Martin Bødtker; Sudano, Isabella; Szucs, Thomas; Adams, Ansgar; ,Extensive carotid atherosclerosis and the diagnostic accuracy of coronary risk calculators,Preventive medicine reports,6,,182-186,2017,Elsevier
Romanensa, Michel; Goerrea, Stefan; Zellwegerb, Michael; Pfistererb, Matthias; ,“Long-term coronary risk in relation to exercise test, SestaMIBI myocardial perfusion, lung uptake, transient ischaemic dilation and left ventricular volumes“,Kardiovaskuläre Medizin,12,4,114-121,2009,
Romanens, M; Darioli, R; ,Carotid Total Plaque Area (TPA): a tool for targeting and evaluating vascular preventive therapy. On behalf of the Taskforceon vascular risk prediction,XVI. Schweizer Atherosklerose-Meeting= XVIe Réunion Suisse d’Athérosclérose,11,,,2008,
Romanens, M; Darioli, R; ,Kardiovaskuläre Risikomarker und Risikofaktoren: Evidenz und Bestimmung: Risikomarker aus Bildgebungsverfahren,Atheroskleroseprävention: Diagnostik und Therapie von Risikofaktoren,,,338-355,2007,Hans Huber
Romanens, Michel; Sudano, Isabella; Szucs, Thomas; Adams, Ansgar; ,Medical costs per QALY of statins based on Swiss Medical Board assumptions,Cardiovascular Medicine,20,04,96-100,2017,EMH Media Spencee, J David; Dariolif, Roger; ,
M. Romanens, A. Adams, I. Sudano, T. Szucs, W. Warmuth; ,Potential for morbidity compression in two healthy population samples. A cross-sectional observation,Cardopvascular Medicine,21,ONLINE APPENDIX,A7,2018,
Romanens, Michel; Szucs, Thomas; Sudano, Isabella; Adams, Ansgar; ,Agreement of PROCAM and SCORE to assess cardiovascular risk in two different low risk European populations,Preventive medicine reports,13,,113,2019,Elsevier
Romanens, Michel; Adams, Ansgar; Estoppey, Laurent; Kurth, Flavian; ,Medical Costs per QALY of Statins Using the Swiss Medical Board (SMB) assumptions: Observed Effects in Two Large Primary Prevention Cohorts from Germany and Switzerland,Athery’s e-pub,,,1-10,2016,
Romanens, Michel; Sudano, Isabella; Adams, Ansgar; Warmuth, Walter; ,“Advanced carotid atherosclerosis in middle-aged subjects: comparison with PROCAM and SCORE risk categories, the potential for reclassification and cost-efficiency of carotid ultrasound in the setting of primary care“,Swiss medical weekly,149,,w20006,2019,EMH Swiss Medical Publishers
Romanens, Michel; Sudano, Isabella; Adams, Ansgar; Schober, Edward A; ,Sonographic assessment of carotid atherosclerosis: preferred risk indicator for future cardiovascular events?,Swiss medical weekly,149,,w20142,2019,EMH Swiss Medical Publishers Adams, Ansgar; Bojara, Waldemar;
Romanens, Michel; ,The determination of the plaque burden on the carotid artery with ultrasound significantly improves the risk prediction in middle-aged subjects compared to PROCAM: an outcome study,Cardiology Research,11,4,233,2020,Elmer Press
Romanens, Michel; Adams, Ansgar; Sudano, Isabella; Bojara, Waldemar; Balint, Sandor; Warmuth, Walter; Szucs, Thomas D; ,Prediction of cardiovascular events with traditional risk equations and total plaque area of carotid atherosclerosis: The Arteris Cardiovascular Outcome (ARCO) cohort study,Preventive Medicine,147,,106525,2021,Academic Press
Romanens, Michel; Adams, Ansgar; Bojara, Waldemar; Balint, Sandor; Warmuth, Walter; ,Cost-effectiveness analysis of statins in primary care: results from the Arteris cohort study,Swiss Medical Weekly,151,1516,w20498-w20498,2021, Adams, Ansgar; Bojara, Waldemar;
Romanens, Michel; ,Effect of statin treatment in patients with advanced carotid atherosclerosis: an observational outcome study,Cardiology Research,12,6,335,2021,Elmer Press
Romanens, Michel; Adams, Ansgar; Warmuth, Walter; ,PROCAM based myocardial infarction risk in relation to global vascular disease risk: observations from the ARCO cohort study,Swiss Medical Weekly,152,0708,w30111-w30111,2022,
Romanens, Michel; Adams, Ansgar; Armando, Luis; Perez, Hernan; Villafañe, Hugo; Garcia, Nestor H; Ibañez, Borja; ,“Reliability, Reproducibility, and Advantages of Measuring Carotid Total Plaque Area“,Journal of the American Society of Echocardiography,35,5,530-532,2022,Elsevier